Dental
Good dental care improves your overall health. Our dental plan is designed to help you maintain a healthy smile through regular dental care and fix any problems as soon as they occur.
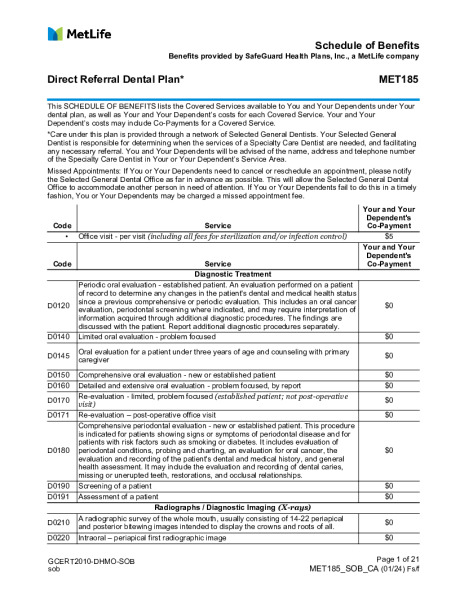
Dental Benefits - HMO
| DHMO | ||
|---|---|---|
| Provider Network | Dental HMO/Managed Care (Met185) | |
| Annual Deductible (Individual/Family) |
$0 | |
| Annual Plan Maximum | $0 | |
| Office Visit – per visit | $5 copay | |
| Diagnostic & Preventive Services | ||
| Oral Evaluation | Covered 100% | |
| Basic Cleanings | Covered 100% | |
| Basic Services | ||
| Amalgam Fillings | Scheduled copays | |
| Root Canal | Scheduled copays | |
| Oral Surgery | Scheduled copays | |
| Major Services | ||
| Crowns | Scheduled copays | |
| Dentures | Scheduled copays | |
| Orthodontic Services | ||
| Orthodontia Lifetime Maximum | $1,695 | |
| Comprehensive Orthodontic Treatment | ||
| Adult | $1,695 | |
| Child | $1,695 | |
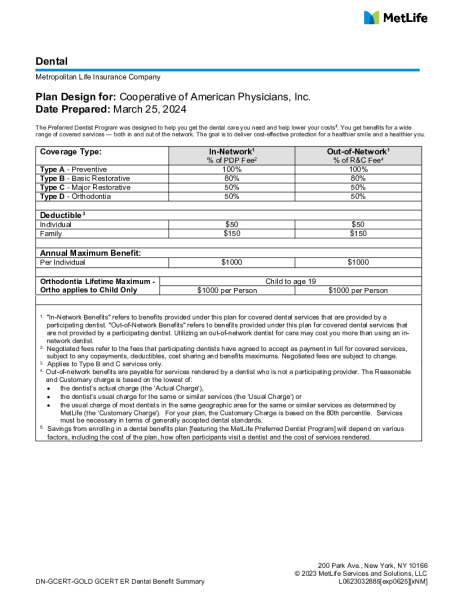
Dental Benefits -PPO
| PPO | ||||
|---|---|---|---|---|
| In-Network | Out-of-Network | |||
| Provider Network | PDP Plus | N/A | ||
| Annual Deductible (Individual/Family) |
$50/$150 | $50/$150 | ||
| Annual Plan Maximum | $1,000 | $1,000 | ||
| Type A - Preventive | ||||
| Oral Evaluation | Covered 100% | Covered 100% | ||
| Basic Cleanings | Covered 100% | Covered 100% | ||
| Type B- Basic Restorative | ||||
| Amalgam Fillings | Covered 80%, After deductible | Covered 80%, After deductible | ||
| Root Canal | Covered 80%, After deductible | Covered 80%, After deductible | ||
| Oral Surgery | Covered 80%, After deductible | Covered 80%, After deductible | ||
| Type C - Major Restorative | ||||
| Crowns | Covered 50%, After deductible | Covered 50%, After deductible | ||
| Dentures | Covered 50%, After deductible | Covered 50%, After deductible | ||
| Type D - Orthodontic Services (Child Only) | ||||
| Orthodontia Lifetime Maximum | $1,000 | $1,000 | ||
| Comprehensive Orthodontic Treatment | ||||
| Adult | Not Covered | Not Covered | ||
| Child | $1,000 | $1,000 | ||
Dental Schedule of Benefits